Background
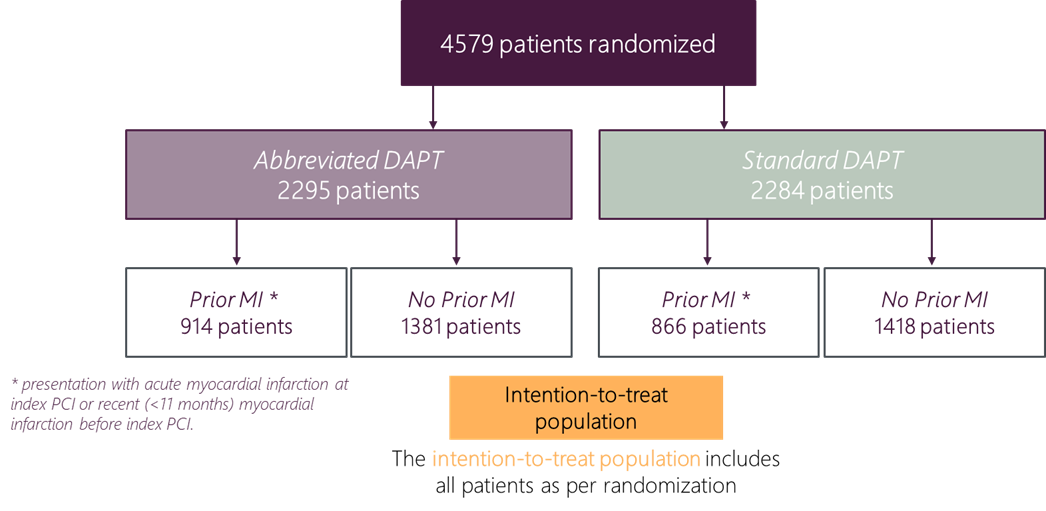
MASTER DAPT was an investigator‑initiated, randomized, controlled, multicenter (n=140), non-inferiority, open‑label trial conducted in patients at high bleeding risk after the implantation of an Ultimaster™/Ultimaster™ Tansei™ DES.
The trial compared abbreviated (1 month) dual antiplatelet therapy (DAPT) with standard (3-12 months) DAPT.
The primary results showed that 1 month of DAPT was non-inferior to treatment continuation for at least 2 additional months for the occurrence of Net Adverse Clinical Events (NACE) and Major Adverse Cardiac and Cerebral Events (MACCE) and significantly reduced Major or Clinically relevant nonmajor Bleeding (MCB) in the overall high bleeding risk population.
Objective
The objective of this prespecified subgroup analysis was to assess, in the high-risk population of patients with a history of acute myocardial infarction in the past 12 months, the consistency of treatment effects between abbreviated and standard DAPT.
Treatment of this patient population can be challenging because of the importance of managing both bleeding and ischemic risk. This population is considered to be at dual risk: a high risk of bleeding on the one hand and a high risk of recurrent ischemic or thrombotic events on the other, so-called "bi-risk" patients.
Methods
Patients randomized to an abbreviated or standard DAPT regimen were grouped according to whether they had a previous infarction within the past 12 months.
Source: C. Smits et al J Am Coll Cardiol. 2022
Results
- NACE and MACCE rates did not differ between an abbreviated (median 34 days) and a non-abbreviated (median 193 days) DAPT strategy.
- There was NO signal towards increased ischemic risk in the abbreviated DAPT population presenting with (recent) acute myocardial infarction.
- An abbreviated APT strategy significantly reduced clinically relevant bleeding risk in these bi-risk patients.
- The abbreviated APT effect was consistent between patients with or without (recent) acute myocardial infarction.
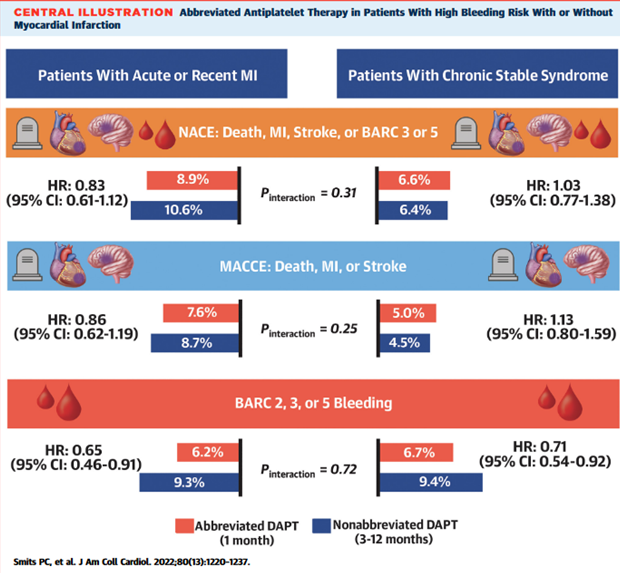
In the stratified subgroup analysis of the multicenter randomized controlled MASTER DAPT (Management of High Bleeding Risk Patients Post Bioresorbable Polymer Coated Stent Implantation With an Abbreviated Versus Standard DAPT Regimen) trial, net adverse clinical outcomes events (NACE) and major adverse cardiac and cerebral events (MACCE) rates did not differ between a 1-month abbreviated dual therapy (DAPT) strategy compared with a nonabbreviated DAPT strategy (3-12 months DAPT) in both subgroups in which patients presented with or without an acute myocardial infarction (MI) or recent history (<11 months) of MI at index percutaneous coronary intervention. The major and nonmajor clinical relevant bleeding rates (Bleeding Academic Research Consortium [BARC]2,3 or 5) were significantly lower with the abbreviated DAPT strategy compared with the nonabbreviated DAPT strategy in both subgroups. NACE was defined as the composite of all-cause death, MI, stroke, and BARC 3 or 5 bleeding. MACCE was defined as the composite of all-cause death, MI, and stroke. BARC is bleeding according to the Bleeding Academic Research Consortium endpoints.
Source: C. Smits et al J Am Coll Cardiol. 2022
Conclusion
One-month DAPT after PCI with the Ultimaster™ Family DES in HBR patients with or without an acute or recent (≤ 12 months) myocardial infarction was associated with:
- Similar Net Adverse Clinical Events (NACE);
- Similar Major Adverse Cardiac or Cerebral Events (MACCE);
- Significantly lower bleeding rates (MCB), without increasing the ischemic risk.
Key Takeaways
These results suggest that it is safe* and beneficial to stop DAPT after 1 month following biodegradable polymer coated sirolimus-eluting coronary stent implantation in patients at HBR presenting with or without an acute or recent (≤12 months) myocardial infarction.
* Stopping DAPT 1-month after coronary stenting was associated with lower bleeding risk and no increased ischemic risk in comparison with continuing DAPT for 2 to 11 months.
Link to the full publication: https://www.jacc.org/doi/10.1016/j.jacc.2022.07.016
