Introducing the patient
Age: 68
Gender: Female
Risk factors for CAD/PAD high blood pressure, diabetes and dyslipenia.
History: Chronical ischemic heart disease and twenty years ago, surgical revascularization in England with double mammary bypass grafts. No medical reports about that surgery were available.
Current presentation: Admitted to the hospital with dyspnoea and syncope after moderate physical effort (walk long distance at the airport).
EKG/echocardiography/angiography/findings:
Coronary angiography and aortography: performed via right common femoral artery (CFA) and an ascendant aorta in “porcelain” was observed with calcifi cation at the abdominal aorta and iliofemoral axis.
Procedure
This porcelain like aorta made the catheters difficult to handle and manipulate. (Fig. 1)
The native coronary arteries and bypass were selectively catheterized. In the native arteries we observed a proximal total occlusion (distal vessel filling by bypass). (Fig. 2 left coronary artery and severely calcified aortic root)
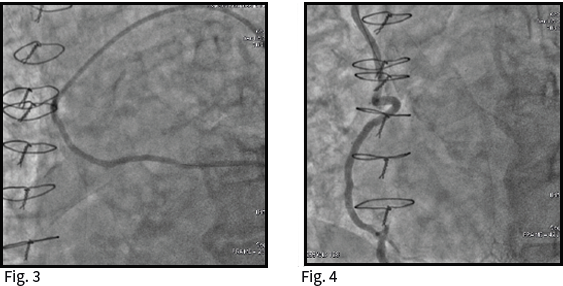
Left mammary was disengaged and a sequential bypass was performed from aorta to intermedium branch and diagonal. This bypass gave flow and filled the left descending artery. (Fig. 3)
Right mammary artery with origin in right subclavian artery and distal anastomosis in right posterior descending artery. (Fig. 4)
Very complex cannulation due to the generalized atherosclerosis and tortuosity in the supra aortic trunks.
Devices
We could not perform the selective injection in the right mammary artery and a PCI guidewire and a thrombus extractor were used in order to make the selective injections through its lumen. Due to the dragged procedure, the use of different catheters, exchange wires, including high support exchange (Amplatz ES) and the need of a PCI guidewire to access the bypass, the catheterization was performed under heparin (8.000 UI).
What happend to the patient?
Immediate procedural outcomes:
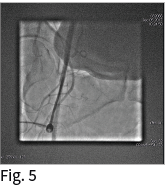
The correct puncture in CFA was verified with an AD30º angiography in the common femoral artery (CFA) (Fig. 5) and the puncture site was closed with a 6F Angio-Seal Evolution (without reverse heparin effect with protamine) ACT value was 185, and the hemostasis was successfully achieved.
No complications were found.
After six hours in bed the patient could sit without bleeding complications, and at 8-10 hours after procedure she started mobilization in her room. She was discharged.
My tips and tricks
Gently place (without applying any pressure) the other hand on the patients groin in order to avoid excessive pulling force on the vessel while you deploy the Angio-Seal system.
Dr. Alfredo Gómez
MD. PHD. Interventional Cardiologist
Hospital Son Espasses. Palma de Mallorca, Spain

